
18 Apr
2012
18 Apr
'12
12:35 p.m.
Eric,
Your comments (pasted in below) to the TRB health and transportation
subcommittee are really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on
non-emergency health transportation systems, which he presented at a
separate workshop around the time of TRB. (He is cc'ed and might have
something to add, as I am not familiar with the specifics of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2
papers for TRB on the subject in the last two years, I am struck by the
lack of access--and not just for patients and visitors, but for employees.
Even our Oakland Kaiser campus, which has a longstanding shuttle service
connecting its buildings to BART, falls pretty short in this area. There is
bike parking in the garage, but it's for employees only and in a dark and
sort of scary place, with no signage or wayfinding. The patient parking
area, when I finally found it, is pretty enough, but very small. And this
from a company whose leadership enthusiastically embraces the 10,000 steps
program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders
themselves, have problems understanding some of the unique needs and
opportunities. (Imagine a changing room, showers and safe and secure bike
parking for staff to avail themselves of lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of
California Transportation Center on 4 Berkeley building owners and their
decisions to invest in this "infrastructure that extends beyond the door."
A policy brief is also attached for quicker reading.
As part of my work developing the CATSIP website on active transportation
safety in California, I also am in contact with bike and ped planners
across the state. Some notable activity is taking place in SF and Silicon
Valley, the latter, I am hearing anecdotally, a hotbed of innovative ways
to incorporate bicycle riding and walking into their campuses (Google,
Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and
opportunities, into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small
shift in design thinking that could alter the fabric of the built
environment to raise awareness of and participation in active
transportation modes (though we would have to evaluate the response to be
certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education
Center<http://www.safetrec.berkeley.edu/>
(SafeTREC)
University of California Transportation Center <http://www.uctc.net/> (UCTC)
Institute for Urban and Regional Development <http://www.iurd.berkeley.edu/>
(IURD)
California Active Transportation Safety Information
Pages<http://catsip.berkeley.edu/>
(CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe <https://twitter.com/#!/transsafe>
@californiaUTC <https://twitter.com/#!/CaliforniaUTC>
@IURDBerkeley <https://twitter.com/#!/IURDBerkeley>
@trbhealth <https://twitter.com/#!/trbhealth>
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber(a)dot.gov>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel
about social determinants of health and health disparities at NIH for
Nation Minority Health Month, I sketched an outline that I think could be
informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough
research being done on bullet #1, while nos 2&3 get covered by a lot of
disciplines. This subcommittee can help fill that gap. There is a need to
look not only at "transportation decisions" which imply planning of
projects & future impacts, but transportation use and availability and
their impact on individual health outcomes. Arguably, transportation has a
much larger impact on health when considered in the immediate term and on
an individual scale.
To use two specific examples: certainly planning decisions can have large
future aggregate impacts on air quality and respiratory health as a result
- but how many people in the past year have ended up in emergency care, or,
sadly, died because they were unable to get to a preventive appointment
like dialysis or other chronic disease treatment? That's a much more
immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit
Analysis of Providing Non-Emergency Medical Transportation,"<
http://www.trb.org/Main/Public/Blurbs/156625.aspx> but this was really only
a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in
the transportation discussion and it's time now to engage more people in
the Health Care & Services sectors. In the long term, I think, that
engagement will have benefits for all of the other questions the
subcommittee considers. As hospitals, insurance companies, and other care
providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation
options and better transportation planning. I mean how many hospitals are
built today to enable, much less encourage, walking to and from? I sure
haven't seen one recently. To what extent to providers consider
transportation access (beyond driving & parking garages) when placing and
planning new facilities? These are all very important issues which are not
being researched.

18 Apr
18 Apr
5:04 p.m.
New subject: [H+T--Friends] active transportation access to health care facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be increased.
But should "changing room, showers" be provided to only one type of commuter? If
they are, they should be carefully costed out, and a conscious decision made to provide
such incentives for bike riders. Or not.
Marc Brenman
----- Original Message -----
From: "Phyllis Orrick" <phylliso(a)berkeley.edu>
To: "erik weber" <erik.weber(a)dot.gov>
Cc: h+t--friends(a)chrispy.net, "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center (SafeTREC)
University of California Transportation Center (UCTC)
Institute for Urban and Regional Development (IURD)
California Active Transportation Safety Information Pages (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@ transsafe
@ californiaUTC
@ IURDBerkeley
@ trbhealth
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: < erik.weber(a)dot.gov >
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's a
much more immediate and measurable impact, yet no one can really say for sure. That's
where, in my opinion, this committee has the biggest opportunity to contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical Transportation,"<
http://www.trb.org/Main/Public/Blurbs/156625.aspx > but this was really only a
beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable, much
less encourage, walking to and from? I sure haven't seen one recently. To what extent
to providers consider transportation access (beyond driving & parking garages) when
placing and planning new facilities? These are all very important issues which are not
being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends

5:20 p.m.
New subject: [H+T--Friends] active transportation access to healthcare facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be
increased. But should "changing room, showers" be provided to only one type of
commuter? If they are, they should be carefully costed out, and a conscious decision made
to provide such incentives for bike riders. Or not.
Marc Brenman
________________________________
From: "Phyllis Orrick" <phylliso(a)berkeley.edu>
To: "erik weber" <erik.weber(a)dot.gov>
Cc: h+t--friends(a)chrispy.net, "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center
<http://www.safetrec.berkeley.edu/> (SafeTREC)
University of California Transportation Center <http://www.uctc.net/> (UCTC)
Institute for Urban and Regional Development <http://www.iurd.berkeley.edu/>
(IURD)
California Active Transportation Safety Information Pages
<http://catsip.berkeley.edu/> (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe <https://twitter.com/#%21/transsafe>
@californiaUTC <https://twitter.com/#%21/CaliforniaUTC>
@IURDBerkeley <https://twitter.com/#%21/IURDBerkeley>
@trbhealth <https://twitter.com/#%21/trbhealth>
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber(a)dot.gov>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's
a much more immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical
Transportation,"<http://www.trb.org/Main/Public/Blurbs/156625.aspx&… but this
was really only a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable,
much less encourage, walking to and from? I sure haven't seen one recently. To what
extent to providers consider transportation access (beyond driving & parking garages)
when placing and planning new facilities? These are all very important issues which are
not being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
6:05 p.m.
New subject: [H+T--Friends] active transportation access to healthcare facilities
Is this really true: " biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: " bicycling for other types of trips – school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments is
probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: " showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
----- Original Message -----
From: "Paula Reeves" <ReevesP(a)wsdot.wa.gov>
To: "TRB Health and Transportation" <h+t--friends(a)chrispy.net>
Cc: "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be increased.
But should "changing room, showers" be provided to only one type of commuter? If
they are, they should be carefully costed out, and a conscious decision made to provide
such incentives for bike riders. Or not.
Marc Brenman
----- Original Message -----
From: "Phyllis Orrick" < phylliso(a)berkeley.edu >
To: "erik weber" < erik.weber(a)dot.gov >
Cc: h+t--friends(a)chrispy.net , "David Ragland" < davidr(a)berkeley.edu >
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center (SafeTREC)
University of California Transportation Center (UCTC)
Institute for Urban and Regional Development (IURD)
California Active Transportation Safety Information Pages (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@ transsafe
@ californiaUTC
@ IURDBerkeley
@ trbhealth
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: < erik.weber(a)dot.gov >
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's a
much more immediate and measurable impact, yet no one can really say for sure. That's
where, in my opinion, this committee has the biggest opportunity to contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical Transportation,"<
http://www.trb.org/Main/Public/Blurbs/156625.aspx > but this was really only a
beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable, much
less encourage, walking to and from? I sure haven't seen one recently. To what extent
to providers consider transportation access (beyond driving & parking garages) when
placing and planning new facilities? These are all very important issues which are not
being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
6:55 p.m.
New subject: [H+T--Friends] active transportation accessto healthcare facilities
In transportation we commonly talk about commute trips. It makes sense for transit and
the public understands rush hour related to their own commute wait times. There may be
other reasons for focusing on commute trips only that I am not aware of. Our national
surveys primarily focus on commute travel at this time and the ACS doesn’t capture enough
data about biking and walking any longer. The NHTS and some regional household surveys
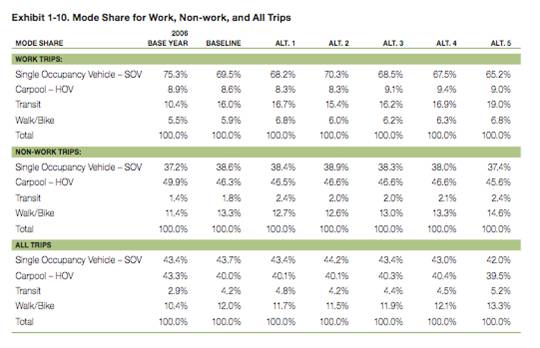
can provide some information about all trips vs. just commute trips. For a breakdown of
the mode share in the Puget Sound Region/Seattle Area based on household travel surveys,
see attached table.
In Washington State, about 5% of all trips are made by transit, while 10% of all miles
traveled and 13% of all trips are made on foot or by bicycle, primarily in urban areas:
about 4% are commute trips; 6% are utilitarian trips like shopping, going to school, or
traveling to medical appointments; and 3% are social or recreational. This makes a lot
of sense when you think about how limited transit services really are. Also, consider
their costs (buses or trains, operating expenses, maintenance).
Biking and walking trips are accommodated at a fraction of the cost of providing other
types of transportation services and building other types of infrastructure. I do combine
biking and walking trips often because infrastructure for one often improves conditions
for the other (i.e., lighting, crossings, trails, showers, lockers, even sidewalk in some
places although not the safest option). Recent studies on ROI back up the logic of making
investments to improve conditions for biking and walking as well. I can provide some ROI
related links and other information.
Good discussion. Look forward to more.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 4:05 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Is this really true: "biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: "bicycling for other types of trips – school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments
is probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: "showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
________________________________
From: "Paula Reeves" <ReevesP(a)wsdot.wa.gov>
To: "TRB Health and Transportation" <h+t--friends(a)chrispy.net>
Cc: "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare
facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be
increased. But should "changing room, showers" be provided to only one type of
commuter? If they are, they should be carefully costed out, and a conscious decision made
to provide such incentives for bike riders. Or not.
Marc Brenman
________________________________
From: "Phyllis Orrick" <phylliso(a)berkeley.edu>
To: "erik weber" <erik.weber(a)dot.gov>
Cc: h+t--friends(a)chrispy.net, "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center
<http://www.safetrec.berkeley.edu/> (SafeTREC)
University of California Transportation Center <http://www.uctc.net/> (UCTC)
Institute for Urban and Regional Development <http://www.iurd.berkeley.edu/>
(IURD)
California Active Transportation Safety Information Pages
<http://catsip.berkeley.edu/> (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe <https://twitter.com/#%21/transsafe>
@californiaUTC <https://twitter.com/#%21/CaliforniaUTC>
@IURDBerkeley <https://twitter.com/#%21/IURDBerkeley>
@trbhealth <https://twitter.com/#%21/trbhealth>
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber(a)dot.gov>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's
a much more immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical
Transportation,"<http://www.trb.org/Main/Public/Blurbs/156625.aspx&… but this
was really only a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable,
much less encourage, walking to and from? I sure haven't seen one recently. To what
extent to providers consider transportation access (beyond driving & parking garages)
when placing and planning new facilities? These are all very important issues which are
not being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
{kind=link}
7:15 p.m.
New subject: [H+T--Friends] active transportationaccessto healthcare facilities
One additional thought for the day - in Washington, mostly urban areas, biking has
increased 116% in the past 5 years. Any other travel trend showing this kind of change
would get a lot of emphasis and a boost in investment. Seems we resist biking, and
walking to a lesser extent, as legitimate travel options.
________________________________
From: h+t--friends-bounces(a)chrispy.net on behalf of Reeves, Paula
Sent: Wed 4/18/2012 4:55 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportationaccessto healthcare facilities
In transportation we commonly talk about commute trips. It makes sense for transit and
the public understands rush hour related to their own commute wait times. There may be
other reasons for focusing on commute trips only that I am not aware of. Our national
surveys primarily focus on commute travel at this time and the ACS doesn't capture
enough data about biking and walking any longer. The NHTS and some regional household
surveys can provide some information about all trips vs. just commute trips. For a
breakdown of the mode share in the Puget Sound Region/Seattle Area based on household
travel surveys, see attached table.
In Washington State, about 5% of all trips are made by transit, while 10% of all miles
traveled and 13% of all trips are made on foot or by bicycle, primarily in urban areas:
about 4% are commute trips; 6% are utilitarian trips like shopping, going to school, or
traveling to medical appointments; and 3% are social or recreational. This makes a lot
of sense when you think about how limited transit services really are. Also, consider
their costs (buses or trains, operating expenses, maintenance).
Biking and walking trips are accommodated at a fraction of the cost of providing other
types of transportation services and building other types of infrastructure. I do combine
biking and walking trips often because infrastructure for one often improves conditions
for the other (i.e., lighting, crossings, trails, showers, lockers, even sidewalk in some
places although not the safest option). Recent studies on ROI back up the logic of making
investments to improve conditions for biking and walking as well. I can provide some ROI
related links and other information.
Good discussion. Look forward to more.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 4:05 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Is this really true: "biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: "bicycling for other types of trips - school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments
is probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: "showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
________________________________
From: "Paula Reeves" <ReevesP(a)wsdot.wa.gov>
To: "TRB Health and Transportation" <h+t--friends(a)chrispy.net>
Cc: "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare
facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips - school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn't have operating cost like transit - much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in 'bike centers' to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be
increased. But should "changing room, showers" be provided to only one type of
commuter? If they are, they should be carefully costed out, and a conscious decision made
to provide such incentives for bike riders. Or not.
Marc Brenman
________________________________
From: "Phyllis Orrick" <phylliso(a)berkeley.edu>
To: "erik weber" <erik.weber(a)dot.gov>
Cc: h+t--friends(a)chrispy.net, "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center
<http://www.safetrec.berkeley.edu/> (SafeTREC)
University of California Transportation Center <http://www.uctc.net/> (UCTC)
Institute for Urban and Regional Development <http://www.iurd.berkeley.edu/>
(IURD)
California Active Transportation Safety Information Pages
<http://catsip.berkeley.edu/> (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe <https://twitter.com/#%21/transsafe>
@californiaUTC <https://twitter.com/#%21/CaliforniaUTC>
@IURDBerkeley <https://twitter.com/#%21/IURDBerkeley>
@trbhealth <https://twitter.com/#%21/trbhealth>
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber(a)dot.gov>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's
a much more immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical
Transportation,"<http://www.trb.org/Main/Public/Blurbs/156625.aspx&… but this
was really only a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable,
much less encourage, walking to and from? I sure haven't seen one recently. To what
extent to providers consider transportation access (beyond driving & parking garages)
when placing and planning new facilities? These are all very important issues which are
not being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
*** eSafe2 scanned this email for malicious content ***
*** IMPORTANT: Do not open attachments from unrecognized senders ***
7:33 p.m.
New subject: [H+T--Friends] active transportation accessto healthcare facilities
Biking and walking are very different. For the statistics to make any sense, they should
be disaggregated. I also disagree that the infrastructure for the two are the same or
similar. Bikers want their own lanes on roads, and are supposed to stay off sidewalks.
Peds don't ask for showers or secure storage. Racial/ethnic breakdowns are different
also; for example, African-Americans walk more, yet one rarely sees an African-American
biker, except for a few young male recreational bikers.
Marc Brenman
----- Original Message -----
From: "Paula Reeves" <ReevesP(a)wsdot.wa.gov>
To: "TRB Health and Transportation" <h+t--friends(a)chrispy.net>
Cc: "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 4:55:48 PM
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
In transportation we commonly talk about commute trips. It makes sense for transit and the
public understands rush hour related to their own commute wait times. There may be other
reasons for focusing on commute trips only that I am not aware of. Our national surveys
primarily focus on commute travel at this time and the ACS doesn’t capture enough data
about biking and walking any longer. The NHTS and some regional household surveys can
provide some information about all trips vs. just commute trips. For a breakdown of the
mode share in the Puget Sound Region/Seattle Area based on household travel surveys, see
attached table.
In Washington State, about 5% of all trips are made by transit, while 10% of all miles
traveled and 13% of all trips are made on foot or by bicycle, primarily in urban areas:
about 4% are commute trips; 6% are utilitarian trips like shopping, going to school, or
traveling to medical appointments; and 3% are social or recreational. This makes a lot of
sense when you think about how limited transit services really are. Also, consider their
costs (buses or trains, operating expenses, maintenance).
Biking and walking trips are accommodated at a fraction of the cost of providing other
types of transportation services and building other types of infrastructure. I do combine
biking and walking trips often because infrastructure for one often improves conditions
for the other (i.e., lighting, crossings, trails, showers, lockers, even sidewalk in some
places although not the safest option). Recent studies on ROI back up the logic of making
investments to improve conditions for biking and walking as well. I can provide some ROI
related links and other information.
Good discussion. Look forward to more.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 4:05 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Is this really true: " biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: "bicycling for other types of trips – school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments is
probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: "showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
----- Original Message -----
From: "Paula Reeves" < ReevesP(a)wsdot.wa.gov >
To: "TRB Health and Transportation" < h+t--friends(a)chrispy.net >
Cc: "David Ragland" < davidr(a)berkeley.edu >
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [ mailto:h+t--friends-bounces@chrispy.net ] On
Behalf Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be increased.
But should "changing room, showers" be provided to only one type of commuter? If
they are, they should be carefully costed out, and a conscious decision made to provide
such incentives for bike riders. Or not.
Marc Brenman
From: "Phyllis Orrick" < phylliso(a)berkeley.edu >
To: "erik weber" < erik.weber(a)dot.gov >
Cc: h+t--friends(a)chrispy.net , "David Ragland" < davidr(a)berkeley.edu >
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center (SafeTREC)
University of California Transportation Center (UCTC)
Institute for Urban and Regional Development (IURD)
California Active Transportation Safety Information Pages (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@ transsafe
@ californiaUTC
@ IURDBerkeley
@ trbhealth
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: < erik.weber(a)dot.gov >
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's a
much more immediate and measurable impact, yet no one can really say for sure. That's
where, in my opinion, this committee has the biggest opportunity to contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical Transportation,"<
http://www.trb.org/Main/Public/Blurbs/156625.aspx > but this was really only a
beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable, much
less encourage, walking to and from? I sure haven't seen one recently. To what extent
to providers consider transportation access (beyond driving & parking garages) when
placing and planning new facilities? These are all very important issues which are not
being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends

19 Apr
19 Apr
7:11 a.m.
New subject: [H+T--Friends] active transportation accessto healthcare facilities
For someone who appears to be quick to ask others to back up any assertion they make with
statistics, you seem to make a number of generalizations about people’s behavior based on
their gender and ethnicity (I am still curious to learn more about all those women
applying make-up and causing dangerous traffic situations).
I do think there’s value in disaggregating statistics for walking and biking, and I hope
this is an area where further research and disaggregation will occur.
RENEE AUTUMN RAY, AICP | Senior Associate | 404.444.6103 (m) |
rray@icfi.com<rray@icfi.com%20> | icfi.com<http://www.icfi.com/>
ICF INTERNATIONAL | 3 Corporate Square NE, Suite 370, Atlanta, GA 30329 | 404.592.2241
(o)
Connect with us on social media<http://www.icfi.com/social>al>.
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 8:34 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Biking and walking are very different. For the statistics to make any sense, they should
be disaggregated. I also disagree that the infrastructure for the two are the same or
similar. Bikers want their own lanes on roads, and are supposed to stay off sidewalks.
Peds don't ask for showers or secure storage. Racial/ethnic breakdowns are different
also; for example, African-Americans walk more, yet one rarely sees an African-American
biker, except for a few young male recreational bikers.
Marc Brenman
________________________________
From: "Paula Reeves"
<ReevesP@wsdot.wa.gov<mailto:ReevesP@wsdot.wa.gov>>
To: "TRB Health and Transportation"
<h+t--friends@chrispy.net<mailto:h+t--friends@chrispy.net>>
Cc: "David Ragland"
<davidr@berkeley.edu<mailto:davidr@berkeley.edu>>
Sent: Wednesday, April 18, 2012 4:55:48 PM
Subject: Re: [H+T--Friends] active transportation accessto healthcare
facilities
In transportation we commonly talk about commute trips. It makes sense for transit and
the public understands rush hour related to their own commute wait times. There may be
other reasons for focusing on commute trips only that I am not aware of. Our national
surveys primarily focus on commute travel at this time and the ACS doesn’t capture enough
data about biking and walking any longer. The NHTS and some regional household surveys
can provide some information about all trips vs. just commute trips. For a breakdown of
the mode share in the Puget Sound Region/Seattle Area based on household travel surveys,
see attached table.
In Washington State, about 5% of all trips are made by transit, while 10% of all miles
traveled and 13% of all trips are made on foot or by bicycle, primarily in urban areas:
about 4% are commute trips; 6% are utilitarian trips like shopping, going to school, or
traveling to medical appointments; and 3% are social or recreational. This makes a lot
of sense when you think about how limited transit services really are. Also, consider
their costs (buses or trains, operating expenses, maintenance).
Biking and walking trips are accommodated at a fraction of the cost of providing other
types of transportation services and building other types of infrastructure. I do combine
biking and walking trips often because infrastructure for one often improves conditions
for the other (i.e., lighting, crossings, trails, showers, lockers, even sidewalk in some
places although not the safest option). Recent studies on ROI back up the logic of making
investments to improve conditions for biking and walking as well. I can provide some ROI
related links and other information.
Good discussion. Look forward to more.
-Paula Reeves
From: h+t--friends-bounces@chrispy.net<mailto:h+t--friends-bounces@chrispy.net>
[mailto:h+t--friends-bounces@chrispy.net]<mailto:[mailto:h+t--friends-bounces@chrispy.net]>
On Behalf Of mbrenman001@comcast.net<mailto:mbrenman001@comcast.net>
Sent: Wednesday, April 18, 2012 4:05 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Is this really true: "biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: "bicycling for other types of trips – school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments
is probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: "showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
________________________________
From: "Paula Reeves"
<ReevesP@wsdot.wa.gov<mailto:ReevesP@wsdot.wa.gov>>
To: "TRB Health and Transportation"
<h+t--friends@chrispy.net<mailto:h+t--friends@chrispy.net>>
Cc: "David Ragland"
<davidr@berkeley.edu<mailto:davidr@berkeley.edu>>
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare
facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces@chrispy.net<mailto:h+t--friends-bounces@chrispy.net>
[mailto:h+t--friends-bounces@chrispy.net] On Behalf Of
mbrenman001@comcast.net<mailto:mbrenman001@comcast.net>
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be
increased. But should "changing room, showers" be provided to only one type of
commuter? If they are, they should be carefully costed out, and a conscious decision made
to provide such incentives for bike riders. Or not.
Marc Brenman
________________________________
From: "Phyllis Orrick"
<phylliso@berkeley.edu<mailto:phylliso@berkeley.edu>>
To: "erik weber" <erik.weber@dot.gov<mailto:erik.weber@dot.gov>>
Cc: h+t--friends@chrispy.net<mailto:h+t--friends@chrispy.net>, "David
Ragland" <davidr@berkeley.edu<mailto:davidr@berkeley.edu>>
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center<http://www.safetrec.berkeley.edu/>
(SafeTREC)
University of California Transportation Center<http://www.uctc.net/> (UCTC)
Institute for Urban and Regional Development<http://www.iurd.berkeley.edu/> (IURD)
California Active Transportation Safety Information
Pages<http://catsip.berkeley.edu/> (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe<https://twitter.com/#%21/transsafe>
@californiaUTC<https://twitter.com/#%21/CaliforniaUTC>
@IURDBerkeley<https://twitter.com/#%21/IURDBerkeley>
@trbhealth<https://twitter.com/#%21/trbhealth>
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber@dot.gov<mailto:erik.weber@dot.gov>>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's
a much more immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical
Transportation,"<http://www.trb.org/Main/Public/Blurbs/156625.aspx&… but this
was really only a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable,
much less encourage, walking to and from? I sure haven't seen one recently. To what
extent to providers consider transportation access (beyond driving & parking garages)
when placing and planning new facilities? These are all very important issues which are
not being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends@ryoko.chrispy.net<mailto:H+T--Friends@ryoko.chrispy.net>
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends@ryoko.chrispy.net<mailto:H+T--Friends@ryoko.chrispy.net>
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends@ryoko.chrispy.net<mailto:H+T--Friends@ryoko.chrispy.net>
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends

8:49 a.m.
New subject: [H+T--Friends] active transportation accessto healthcare facilities
Those sound a lot like anecdotal conjectures to me, Marc. The data shows they’re poor
conjectures, too:
NHTSA found in 2002 that 78.6% of non-Hispanic whites had walked in the past 30 days,
while only 75.5% of non-Hispanic blacks had. Whites averaged 1.6 trips per day by walking
while blacks averaged a slightly higher 1.9 trips.
http://www.bts.gov/programs/omnibus_surveys/targeted_survey/2002_national_s…
For biking, blacks actually took more trips per day by bike than whites:
[cid:image001.png@01CD1E11.C6A28770]
http://www.bts.gov/programs/omnibus_surveys/targeted_survey/2002_national_s…
The white guys in spandex on bikes trope has been disproven many times. They may be the
more prevalent on the recreational trail on weekends, or making the commute through
downtown, but that doesn’t mean they’re the only people riding bicycles.
Erik Weber
United We Ride
Office of Program Management
FTA – USDOT
Ph: 202.366.0705
P Please consider the environment before printing this email.
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 8:34 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Biking and walking are very different. For the statistics to make any sense, they should
be disaggregated. I also disagree that the infrastructure for the two are the same or
similar. Bikers want their own lanes on roads, and are supposed to stay off sidewalks.
Peds don't ask for showers or secure storage. Racial/ethnic breakdowns are different
also; for example, African-Americans walk more, yet one rarely sees an African-American
biker, except for a few young male recreational bikers.
Marc Brenman
________________________________
From: "Paula Reeves"
<ReevesP@wsdot.wa.gov<mailto:ReevesP@wsdot.wa.gov>>
To: "TRB Health and Transportation"
<h+t--friends@chrispy.net<mailto:h+t--friends@chrispy.net>>
Cc: "David Ragland"
<davidr@berkeley.edu<mailto:davidr@berkeley.edu>>
Sent: Wednesday, April 18, 2012 4:55:48 PM
Subject: Re: [H+T--Friends] active transportation accessto healthcare
facilities
In transportation we commonly talk about commute trips. It makes sense for transit and
the public understands rush hour related to their own commute wait times. There may be
other reasons for focusing on commute trips only that I am not aware of. Our national
surveys primarily focus on commute travel at this time and the ACS doesn’t capture enough
data about biking and walking any longer. The NHTS and some regional household surveys
can provide some information about all trips vs. just commute trips. For a breakdown of
the mode share in the Puget Sound Region/Seattle Area based on household travel surveys,
see attached table.
In Washington State, about 5% of all trips are made by transit, while 10% of all miles
traveled and 13% of all trips are made on foot or by bicycle, primarily in urban areas:
about 4% are commute trips; 6% are utilitarian trips like shopping, going to school, or
traveling to medical appointments; and 3% are social or recreational. This makes a lot
of sense when you think about how limited transit services really are. Also, consider
their costs (buses or trains, operating expenses, maintenance).
Biking and walking trips are accommodated at a fraction of the cost of providing other
types of transportation services and building other types of infrastructure. I do combine
biking and walking trips often because infrastructure for one often improves conditions
for the other (i.e., lighting, crossings, trails, showers, lockers, even sidewalk in some
places although not the safest option). Recent studies on ROI back up the logic of making
investments to improve conditions for biking and walking as well. I can provide some ROI
related links and other information.
Good discussion. Look forward to more.
-Paula Reeves
From: h+t--friends-bounces@chrispy.net<mailto:h+t--friends-bounces@chrispy.net>
[mailto:h+t--friends-bounces@chrispy.net]<mailto:[mailto:h+t--friends-bounces@chrispy.net]>
On Behalf Of mbrenman001@comcast.net<mailto:mbrenman001@comcast.net>
Sent: Wednesday, April 18, 2012 4:05 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Is this really true: "biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: "bicycling for other types of trips – school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments
is probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: "showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
________________________________
From: "Paula Reeves"
<ReevesP@wsdot.wa.gov<mailto:ReevesP@wsdot.wa.gov>>
To: "TRB Health and Transportation"
<h+t--friends@chrispy.net<mailto:h+t--friends@chrispy.net>>
Cc: "David Ragland"
<davidr@berkeley.edu<mailto:davidr@berkeley.edu>>
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare
facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces@chrispy.net<mailto:h+t--friends-bounces@chrispy.net>
[mailto:h+t--friends-bounces@chrispy.net] On Behalf Of
mbrenman001@comcast.net<mailto:mbrenman001@comcast.net>
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be
increased. But should "changing room, showers" be provided to only one type of
commuter? If they are, they should be carefully costed out, and a conscious decision made
to provide such incentives for bike riders. Or not.
Marc Brenman
________________________________
From: "Phyllis Orrick"
<phylliso@berkeley.edu<mailto:phylliso@berkeley.edu>>
To: "erik weber" <erik.weber@dot.gov<mailto:erik.weber@dot.gov>>
Cc: h+t--friends@chrispy.net<mailto:h+t--friends@chrispy.net>, "David
Ragland" <davidr@berkeley.edu<mailto:davidr@berkeley.edu>>
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center<http://www.safetrec.berkeley.edu/>
(SafeTREC)
University of California Transportation Center<http://www.uctc.net/> (UCTC)
Institute for Urban and Regional Development<http://www.iurd.berkeley.edu/> (IURD)
California Active Transportation Safety Information
Pages<http://catsip.berkeley.edu/> (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe<https://twitter.com/#%21/transsafe>
@californiaUTC<https://twitter.com/#%21/CaliforniaUTC>
@IURDBerkeley<https://twitter.com/#%21/IURDBerkeley>
@trbhealth<https://twitter.com/#%21/trbhealth>
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber@dot.gov<mailto:erik.weber@dot.gov>>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's
a much more immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical
Transportation,"<http://www.trb.org/Main/Public/Blurbs/156625.aspx&… but this
was really only a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable,
much less encourage, walking to and from? I sure haven't seen one recently. To what
extent to providers consider transportation access (beyond driving & parking garages)
when placing and planning new facilities? These are all very important issues which are
not being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends@ryoko.chrispy.net<mailto:H+T--Friends@ryoko.chrispy.net>
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends@ryoko.chrispy.net<mailto:H+T--Friends@ryoko.chrispy.net>
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends@ryoko.chrispy.net<mailto:H+T--Friends@ryoko.chrispy.net>
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
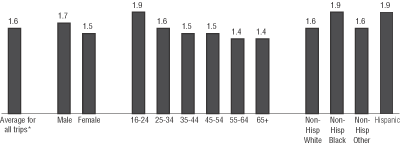{kind=link}
10:22 a.m.
New subject: [H+T--Friends] active transportation accessto healthcare facilities
Thanks for sharing this Eric. I think the socio-economic data on travel – particularly
for all trip types - is limited and one area in need of more research and evaluation.
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of erik.weber(a)dot.gov
Sent: Thursday, April 19, 2012 6:50 AM
To: h+t--friends(a)chrispy.net
Cc: davidr(a)berkeley.edu
Subject: Re: [H+T--Friends]active transportation accessto healthcare facilities
Those sound a lot like anecdotal conjectures to me, Marc. The data shows they’re poor
conjectures, too:
NHTSA found in 2002 that 78.6% of non-Hispanic whites had walked in the past 30 days,
while only 75.5% of non-Hispanic blacks had. Whites averaged 1.6 trips per day by walking
while blacks averaged a slightly higher 1.9 trips.
http://www.bts.gov/programs/omnibus_surveys/targeted_survey/2002_national_s…
For biking, blacks actually took more trips per day by bike than whites:
http://www.bts.gov/programs/omnibus_surveys/targeted_survey/2002_national_s…
The white guys in spandex on bikes trope has been disproven many times. They may be the
more prevalent on the recreational trail on weekends, or making the commute through
downtown, but that doesn’t mean they’re the only people riding bicycles.
Erik Weber
United We Ride
Office of Program Management
FTA – USDOT
Ph: 202.366.0705
P Please consider the environment before printing this email.
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 8:34 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Biking and walking are very different. For the statistics to make any sense, they should
be disaggregated. I also disagree that the infrastructure for the two are the same or
similar. Bikers want their own lanes on roads, and are supposed to stay off sidewalks.
Peds don't ask for showers or secure storage. Racial/ethnic breakdowns are different
also; for example, African-Americans walk more, yet one rarely sees an African-American
biker, except for a few young male recreational bikers.
Marc Brenman
________________________________
From: "Paula Reeves" <ReevesP(a)wsdot.wa.gov>
To: "TRB Health and Transportation" <h+t--friends(a)chrispy.net>
Cc: "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 4:55:48 PM
Subject: Re: [H+T--Friends] active transportation accessto healthcare
facilities
In transportation we commonly talk about commute trips. It makes sense for transit and
the public understands rush hour related to their own commute wait times. There may be
other reasons for focusing on commute trips only that I am not aware of. Our national
surveys primarily focus on commute travel at this time and the ACS doesn’t capture enough
data about biking and walking any longer. The NHTS and some regional household surveys
can provide some information about all trips vs. just commute trips. For a breakdown of
the mode share in the Puget Sound Region/Seattle Area based on household travel surveys,
see attached table.
In Washington State, about 5% of all trips are made by transit, while 10% of all miles
traveled and 13% of all trips are made on foot or by bicycle, primarily in urban areas:
about 4% are commute trips; 6% are utilitarian trips like shopping, going to school, or
traveling to medical appointments; and 3% are social or recreational. This makes a lot
of sense when you think about how limited transit services really are. Also, consider
their costs (buses or trains, operating expenses, maintenance).
Biking and walking trips are accommodated at a fraction of the cost of providing other
types of transportation services and building other types of infrastructure. I do combine
biking and walking trips often because infrastructure for one often improves conditions
for the other (i.e., lighting, crossings, trails, showers, lockers, even sidewalk in some
places although not the safest option). Recent studies on ROI back up the logic of making
investments to improve conditions for biking and walking as well. I can provide some ROI
related links and other information.
Good discussion. Look forward to more.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 4:05 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Is this really true: "biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: "bicycling for other types of trips – school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments
is probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: "showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
________________________________
From: "Paula Reeves" <ReevesP(a)wsdot.wa.gov>
To: "TRB Health and Transportation" <h+t--friends(a)chrispy.net>
Cc: "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare
facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be
increased. But should "changing room, showers" be provided to only one type of
commuter? If they are, they should be carefully costed out, and a conscious decision made
to provide such incentives for bike riders. Or not.
Marc Brenman
________________________________
From: "Phyllis Orrick" <phylliso(a)berkeley.edu>
To: "erik weber" <erik.weber(a)dot.gov>
Cc: h+t--friends(a)chrispy.net, "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center
<http://www.safetrec.berkeley.edu/> (SafeTREC)
University of California Transportation Center <http://www.uctc.net/> (UCTC)
Institute for Urban and Regional Development <http://www.iurd.berkeley.edu/>
(IURD)
California Active Transportation Safety Information Pages
<http://catsip.berkeley.edu/> (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe <https://twitter.com/#%21/transsafe>
@californiaUTC <https://twitter.com/#%21/CaliforniaUTC>
@IURDBerkeley <https://twitter.com/#%21/IURDBerkeley>
@trbhealth <https://twitter.com/#%21/trbhealth>
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber(a)dot.gov>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's
a much more immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical
Transportation,"<http://www.trb.org/Main/Public/Blurbs/156625.aspx&… but this
was really only a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable,
much less encourage, walking to and from? I sure haven't seen one recently. To what
extent to providers consider transportation access (beyond driving & parking garages)
when placing and planning new facilities? These are all very important issues which are
not being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
*** eSafe2 scanned this email for malicious content ***
*** IMPORTANT: Do not open attachments from unrecognized senders ***
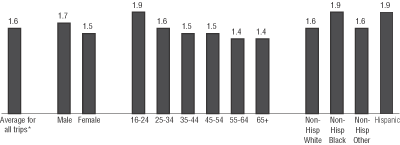{kind=link}
24 Apr
24 Apr
9:41 a.m.
New subject: [H+T--Friends] active transportation accessto healthcare facilities
The difference here is hardly trivial and certainly not "slightly": "
Whites averaged 1.6 trips per day by walking while blacks averaged a slightly higher 1.9
trips." That's 19% more walking for Blacks.
I am completely befuddled by the alleged statistics on Black bicycle riders. I just
don't see them. Where are they? As a social equity worker, I'm kind of a
professional nose counter. It makes me wonder about how the survey cited was taken.
Marc Brenman
----- Original Message -----
From: "erik weber" <erik.weber(a)dot.gov>
To: h+t--friends(a)chrispy.net
Cc: davidr(a)berkeley.edu
Sent: Thursday, April 19, 2012 6:49:57 AM
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Those sound a lot like anecdotal conjectures to me, Marc. The data shows they’re poor
conjectures, too:
NHTSA found in 2002 that 78.6% of non-Hispanic whites had walked in the past 30 days,
while only 75.5% of non-Hispanic blacks had. Whites averaged 1.6 trips per day by walking
while blacks averaged a slightly higher 1.9 trips.
http://www.bts.gov/programs/omnibus_surveys/targeted_survey/2002_national_s…
For biking, blacks actually took more trips per day by bike than whites:
http://www.bts.gov/programs/omnibus_surveys/targeted_survey/2002_national_s…
The white guys in spandex on bikes trope has been disproven many times. They may be the
more prevalent on the recreational trail on weekends, or making the commute through
downtown, but that doesn’t mean they’re the only people riding bicycles.
Erik Weber
United We Ride
Office of Program Management
FTA – USDOT
Ph: 202.366.0705
P Please consider the environment before printing this email.
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 8:34 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Biking and walking are very different. For the statistics to make any sense, they should
be disaggregated. I also disagree that the infrastructure for the two are the same or
similar. Bikers want their own lanes on roads, and are supposed to stay off sidewalks.
Peds don't ask for showers or secure storage. Racial/ethnic breakdowns are different
also; for example, African-Americans walk more, yet one rarely sees an African-American
biker, except for a few young male recreational bikers.
Marc Brenman
----- Original Message -----
From: "Paula Reeves" < ReevesP(a)wsdot.wa.gov >
To: "TRB Health and Transportation" < h+t--friends(a)chrispy.net >
Cc: "David Ragland" < davidr(a)berkeley.edu >
Sent: Wednesday, April 18, 2012 4:55:48 PM
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
In transportation we commonly talk about commute trips. It makes sense for transit and the
public understands rush hour related to their own commute wait times. There may be other
reasons for focusing on commute trips only that I am not aware of. Our national surveys
primarily focus on commute travel at this time and the ACS doesn’t capture enough data
about biking and walking any longer. The NHTS and some regional household surveys can
provide some information about all trips vs. just commute trips. For a breakdown of the
mode share in the Puget Sound Region/Seattle Area based on household travel surveys, see
attached table.
In Washington State, about 5% of all trips are made by transit, while 10% of all miles
traveled and 13% of all trips are made on foot or by bicycle, primarily in urban areas:
about 4% are commute trips; 6% are utilitarian trips like shopping, going to school, or
traveling to medical appointments; and 3% are social or recreational. This makes a lot of
sense when you think about how limited transit services really are. Also, consider their
costs (buses or trains, operating expenses, maintenance).
Biking and walking trips are accommodated at a fraction of the cost of providing other
types of transportation services and building other types of infrastructure. I do combine
biking and walking trips often because infrastructure for one often improves conditions
for the other (i.e., lighting, crossings, trails, showers, lockers, even sidewalk in some
places although not the safest option). Recent studies on ROI back up the logic of making
investments to improve conditions for biking and walking as well. I can provide some ROI
related links and other information.
Good discussion. Look forward to more.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 4:05 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Is this really true: " biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: "bicycling for other types of trips – school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments is
probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: "showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
From: "Paula Reeves" < ReevesP(a)wsdot.wa.gov >
To: "TRB Health and Transportation" < h+t--friends(a)chrispy.net >
Cc: "David Ragland" < davidr(a)berkeley.edu >
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [ mailto:h+t--friends-bounces@chrispy.net ] On
Behalf Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be increased.
But should "changing room, showers" be provided to only one type of commuter? If
they are, they should be carefully costed out, and a conscious decision made to provide
such incentives for bike riders. Or not.
Marc Brenman
From: "Phyllis Orrick" < phylliso(a)berkeley.edu >
To: "erik weber" < erik.weber(a)dot.gov >
Cc: h+t--friends(a)chrispy.net , "David Ragland" < davidr(a)berkeley.edu >
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center (SafeTREC)
University of California Transportation Center (UCTC)
Institute for Urban and Regional Development (IURD)
California Active Transportation Safety Information Pages (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@ transsafe
@ californiaUTC
@ IURDBerkeley
@ trbhealth
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: < erik.weber(a)dot.gov >
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's a
much more immediate and measurable impact, yet no one can really say for sure. That's
where, in my opinion, this committee has the biggest opportunity to contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical Transportation,"<
http://www.trb.org/Main/Public/Blurbs/156625.aspx > but this was really only a
beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable, much
less encourage, walking to and from? I sure haven't seen one recently. To what extent
to providers consider transportation access (beyond driving & parking garages) when
placing and planning new facilities? These are all very important issues which are not
being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
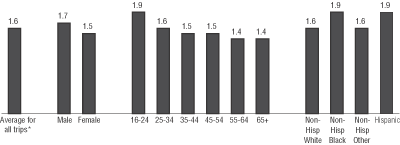{kind=link}
19 Apr
19 Apr
10:18 a.m.
New subject: [H+T--Friends] active transportation access to healthcare facilities
I should clarify – I agree that biking and walking are different. However, in terms of
infrastructure (the majority of the investment to accommodate both modes), improving
conditions for biking can often improve conditions for walking and vice versa. This is
founded in research we have done here at WSDOT and national studies. For example,
installing a bike lane in the street or road provides additional buffer for pedestrians
and can slow motor vehicles. Installing lighting improves conditions for both.
Installing medians improves conditions for both, as well as signals, sidewalks, trails,
signage. In most cities in Washington, biking on sidewalks is permitted. Although, I
agree that isn’t the safest option as someone who was hit by a backing vehicle on the
sidewalk.
I have worked on Washington’s Commute Trip Reduction program extensively and found through
our employment site surveys that pedestrians request lockers and showers and appreciate
that sort of accommodation as much if not more than cyclists. So, I disagree on that
point.
Regarding the racial and ethnic breakdowns, I think more research is needed. These
numbers are changing rapidly these past few years. If you have data for some of the
points you made below, please share it. We are very interested.
Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 5:34 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] activetransportation accessto healthcare facilities
Biking and walking are very different. For the statistics to make any sense, they should
be disaggregated. I also disagree that the infrastructure for the two are the same or
similar. Bikers want their own lanes on roads, and are supposed to stay off sidewalks.
Peds don't ask for showers or secure storage. Racial/ethnic breakdowns are different
also; for example, African-Americans walk more, yet one rarely sees an African-American
biker, except for a few young male recreational bikers.
Marc Brenman
________________________________
From: "Paula Reeves" <ReevesP(a)wsdot.wa.gov>
To: "TRB Health and Transportation" <h+t--friends(a)chrispy.net>
Cc: "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 4:55:48 PM
Subject: Re: [H+T--Friends] active transportation accessto healthcare
facilities
In transportation we commonly talk about commute trips. It makes sense for transit and
the public understands rush hour related to their own commute wait times. There may be
other reasons for focusing on commute trips only that I am not aware of. Our national
surveys primarily focus on commute travel at this time and the ACS doesn’t capture enough
data about biking and walking any longer. The NHTS and some regional household surveys
can provide some information about all trips vs. just commute trips. For a breakdown of
the mode share in the Puget Sound Region/Seattle Area based on household travel surveys,
see attached table.
In Washington State, about 5% of all trips are made by transit, while 10% of all miles
traveled and 13% of all trips are made on foot or by bicycle, primarily in urban areas:
about 4% are commute trips; 6% are utilitarian trips like shopping, going to school, or
traveling to medical appointments; and 3% are social or recreational. This makes a lot
of sense when you think about how limited transit services really are. Also, consider
their costs (buses or trains, operating expenses, maintenance).
Biking and walking trips are accommodated at a fraction of the cost of providing other
types of transportation services and building other types of infrastructure. I do combine
biking and walking trips often because infrastructure for one often improves conditions
for the other (i.e., lighting, crossings, trails, showers, lockers, even sidewalk in some
places although not the safest option). Recent studies on ROI back up the logic of making
investments to improve conditions for biking and walking as well. I can provide some ROI
related links and other information.
Good discussion. Look forward to more.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 4:05 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation accessto healthcare facilities
Is this really true: "biking and walking trips exceed transit trips in many
places." Can anyone provide me some cites to this effect? I would guess that these
bike uses are extremely small: "bicycling for other types of trips – school,
shopping, social, medical etc." In fact, the use of bikes for medical appointments
is probably vanishingly small. Similarly with bikes for shopping other than very light
shopping. Or is my confusion due to the lumping of biking and walking, which are very
different? By the way, these features cost money: "showers, lockers, repair
facilities" and secure storage facilities.
Marc Brenman
________________________________
From: "Paula Reeves" <ReevesP(a)wsdot.wa.gov>
To: "TRB Health and Transportation" <h+t--friends(a)chrispy.net>
Cc: "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 3:20:46 PM
Subject: Re: [H+T--Friends] active transportation access to healthcare
facilities
While the percent of bike commuters is relatively small, bicycling for other types of
trips – school, shopping, social, medical etc.. are important to consider. Together,
biking and walking trips exceed transit trips in many places. Accommodating biking and
walking trips doesn’t have operating cost like transit – much lower per trip cost for
biking and walking. Features like showers, lockers, repair facilities, etc can often be
combined in ‘bike centers’ to make the most of these investments.
-Paula Reeves
From: h+t--friends-bounces(a)chrispy.net [mailto:h+t--friends-bounces@chrispy.net] On Behalf
Of mbrenman001(a)comcast.net
Sent: Wednesday, April 18, 2012 3:04 PM
To: TRB Health and Transportation
Cc: David Ragland
Subject: Re: [H+T--Friends] active transportation access to healthcare facilities
At the moment, the percent of bike riders to work is tiny. Perhaps it should be
increased. But should "changing room, showers" be provided to only one type of
commuter? If they are, they should be carefully costed out, and a conscious decision made
to provide such incentives for bike riders. Or not.
Marc Brenman
________________________________
From: "Phyllis Orrick" <phylliso(a)berkeley.edu>
To: "erik weber" <erik.weber(a)dot.gov>
Cc: h+t--friends(a)chrispy.net, "David Ragland" <davidr(a)berkeley.edu>
Sent: Wednesday, April 18, 2012 10:35:31 AM
Subject: [H+T--Friends] active transportation access to health care facilities
Eric,
Your comments (pasted in below) to the TRB health and transportation subcommittee are
really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on non-emergency health
transportation systems, which he presented at a separate workshop around the time of TRB.
(He is cc'ed and might have something to add, as I am not familiar with the specifics
of his findings.)
In terms of health care facilities' "friendliness" to active transportation
access, as someone who thinks about bicycle-oriented design and has done 2 papers for TRB
on the subject in the last two years, I am struck by the lack of access--and not just for
patients and visitors, but for employees. Even our Oakland Kaiser campus, which has a
longstanding shuttle service connecting its buildings to BART, falls pretty short in this
area. There is bike parking in the garage, but it's for employees only and in a dark
and sort of scary place, with no signage or wayfinding. The patient parking area, when I
finally found it, is pretty enough, but very small. And this from a company whose
leadership enthusiastically embraces the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders themselves,
have problems understanding some of the unique needs and opportunities. (Imagine a
changing room, showers and safe and secure bike parking for staff to avail themselves of
lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of California
Transportation Center on 4 Berkeley building owners and their decisions to invest in this
"infrastructure that extends beyond the door." A policy brief is also attached
for quicker reading.
As part of my work developing the CATSIP website on active transportation safety in
California, I also am in contact with bike and ped planners across the state. Some notable
activity is taking place in SF and Silicon Valley, the latter, I am hearing anecdotally, a
hotbed of innovative ways to incorporate bicycle riding and walking into their campuses
(Google, Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and opportunities,
into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small shift in design
thinking that could alter the fabric of the built environment to raise awareness of and
participation in active transportation modes (though we would have to evaluate the
response to be certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education Center
<http://www.safetrec.berkeley.edu/> (SafeTREC)
University of California Transportation Center <http://www.uctc.net/> (UCTC)
Institute for Urban and Regional Development <http://www.iurd.berkeley.edu/>
(IURD)
California Active Transportation Safety Information Pages
<http://catsip.berkeley.edu/> (CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe <https://twitter.com/#%21/transsafe>
@californiaUTC <https://twitter.com/#%21/CaliforniaUTC>
@IURDBerkeley <https://twitter.com/#%21/IURDBerkeley>
@trbhealth <https://twitter.com/#%21/trbhealth>
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber(a)dot.gov>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel about social
determinants of health and health disparities at NIH for Nation Minority Health Month, I
sketched an outline that I think could be informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough research being
done on bullet #1, while nos 2&3 get covered by a lot of disciplines. This
subcommittee can help fill that gap. There is a need to look not only at
"transportation decisions" which imply planning of projects & future
impacts, but transportation use and availability and their impact on individual health
outcomes. Arguably, transportation has a much larger impact on health when considered in
the immediate term and on an individual scale.
To use two specific examples: certainly planning decisions can have large future aggregate
impacts on air quality and respiratory health as a result - but how many people in the
past year have ended up in emergency care, or, sadly, died because they were unable to get
to a preventive appointment like dialysis or other chronic disease treatment? That's
a much more immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit Analysis of
Providing Non-Emergency Medical
Transportation,"<http://www.trb.org/Main/Public/Blurbs/156625.aspx&… but this
was really only a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in the
transportation discussion and it's time now to engage more people in the Health Care
& Services sectors. In the long term, I think, that engagement will have benefits for
all of the other questions the subcommittee considers. As hospitals, insurance companies,
and other care providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation options and
better transportation planning. I mean how many hospitals are built today to enable,
much less encourage, walking to and from? I sure haven't seen one recently. To what
extent to providers consider transportation access (beyond driving & parking garages)
when placing and planning new facilities? These are all very important issues which are
not being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends

7:33 a.m.
Wow, it strikes me that after only a couple of generations of auto-oriented
culture and design, we have completely forgotten how to integrate
non-automobile access and networks and treat hundreds of years of street
design as if it never happened.
All through pregnancy, I walked to Beth Israel Medical Center in New York past
Union Square from the subway or the express bus. Yes, this is a 19th
century grid, but it can be easily replicated. It works, keeping New
Yorkers walking and healthy. There are lots of other examples.
Bike and pedestrian access is not difficult to design as long as the
commitment is there on the part of those involved in funding and building.
Just a little rant to start the day.
On Wed, Apr 18, 2012 at 1:35 PM, Phyllis Orrick <phylliso(a)berkeley.edu>wrote;wrote:
Eric,
Your comments (pasted in below) to the TRB health and transportation
subcommittee are really interesting and useful.
David Ragland, here at SafeTREC, has done some preliminary work on
non-emergency health transportation systems, which he presented at a
separate workshop around the time of TRB. (He is cc'ed and might have
something to add, as I am not familiar with the specifics of his findings.)
In terms of health care facilities' "friendliness" to active
transportation access, as someone who thinks about bicycle-oriented design
and has done 2 papers for TRB on the subject in the last two years, I am
struck by the lack of access--and not just for patients and visitors, but
for employees. Even our Oakland Kaiser campus, which has a longstanding
shuttle service connecting its buildings to BART, falls pretty short in
this area. There is bike parking in the garage, but it's for employees only
and in a dark and sort of scary place, with no signage or wayfinding. The
patient parking area, when I finally found it, is pretty enough, but very
small. And this from a company whose leadership enthusiastically embraces
the 10,000 steps program.
Part of the difficulty is that building owners and operators don't have a
"cookbook" for these designs and, unless they are bicycle riders
themselves, have problems understanding some of the unique needs and
opportunities. (Imagine a changing room, showers and safe and secure bike
parking for staff to avail themselves of lunchbreak bike rides.)
I'm attaching a paper I did with Karen Frick of the University of
California Transportation Center on 4 Berkeley building owners and their
decisions to invest in this "infrastructure that extends beyond the door."
A policy brief is also attached for quicker reading.
As part of my work developing the CATSIP website on active transportation
safety in California, I also am in contact with bike and ped planners
across the state. Some notable activity is taking place in SF and Silicon
Valley, the latter, I am hearing anecdotally, a hotbed of innovative ways
to incorporate bicycle riding and walking into their campuses (Google,
Facebook and Apple, to name a few). I can't help but think it would be of
value to collect their design solutions, along with costs, challenges and
opportunities, into a central toolkit.
Anyway, sorry for the long comments, but it seems like a potentially small
shift in design thinking that could alter the fabric of the built
environment to raise awareness of and participation in active
transportation modes (though we would have to evaluate the response to be
certain).
Best,
Phyllis
--
Communications Director
Safe Transportation Research and Education
Center<http://www.safetrec.berkeley.edu/>
(SafeTREC)
University of California Transportation Center <http://www.uctc.net/>
(UCTC)
Institute for Urban and Regional Development<http://www.iurd.berkeley.edu/>
(IURD)
California Active Transportation Safety Information
Pages<http://catsip.berkeley.edu/>
(CATSIP)
2614 Dwight Way
UC Berkeley
Berkeley CA 94720-7374
510-643-1779
@transsafe <https://twitter.com/#%21/transsafe>
@californiaUTC <https://twitter.com/#%21/CaliforniaUTC>
@IURDBerkeley <https://twitter.com/#%21/IURDBerkeley>
@trbhealth <https://twitter.com/#%21/trbhealth>
--
Sheryl Gross-Glaser
Director, Partnership for Mobility Management
Coordination Specialist, National Resource Center for Human Service
Transportation Coordination
Community Transportation Association of America
grossglaser(a)ctaa.org
202.386.1669
<http://www.NRCtransportation.org>*** *** ***
The Express Stop: <http://www.NRCtransportation.org>
http://express-stop.blogspot.com/
NRC Technical Assistance News: http://nrctanews.blogspot.com/
www.NRCtransportation.org
partnershipformobilitymanagement.org
www.ctaa.org
CTAA EXPO at Baltimore's Inner Harbor
May 20-25, 2012
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
From: <erik.weber(a)dot.gov>
Subject: Re: [H+T--Friends] Help inform our Subcommittee's TRB 2013
Workshop Proposal!
In preparing a DOT presentation on Transportation and Health at a panel
about social determinants of health and health disparities at NIH for
Nation Minority Health Month, I sketched an outline that I think could be
informative to planning next year:
Transportation's impact on health
* Transportation availability & access to care
* Transportation options & livable communities
* Transportation planning & environmental justice
As I mentioned back at the annual meeting, there is nowhere near enough
research being done on bullet #1, while nos 2&3 get covered by a lot of
disciplines. This subcommittee can help fill that gap. There is a need to
look not only at "transportation decisions" which imply planning of
projects & future impacts, but transportation use and availability and
their impact on individual health outcomes. Arguably, transportation has a
much larger impact on health when considered in the immediate term and on
an individual scale.
To use two specific examples: certainly planning decisions can have large
future aggregate impacts on air quality and respiratory health as a result
- but how many people in the past year have ended up in emergency care, or,
sadly, died because they were unable to get to a preventive appointment
like dialysis or other chronic disease treatment? That's a much more
immediate and measurable impact, yet no one can really say for sure.
That's where, in my opinion, this committee has the biggest opportunity to
contribute.
I think TCRP made a good foray into this area with B-27 "Cost Benefit
Analysis of Providing Non-Emergency Medical Transportation,"<
http://www.trb.org/Main/Public/Blurbs/156625.aspx> but this was really
only a beginning, and happened 7 years ago now.
I would argue that the Public Health sector is pretty strongly engaged in
the transportation discussion and it's time now to engage more people in
the Health Care & Services sectors. In the long term, I think, that
engagement will have benefits for all of the other questions the
subcommittee considers. As hospitals, insurance companies, and other care
providers better understand the direct impact of transportation on their
missions and their bottom lines, the more they will support transportation
options and better transportation planning. I mean how many hospitals are
built today to enable, much less encourage, walking to and from? I sure
haven't seen one recently. To what extent to providers consider
transportation access (beyond driving & parking garages) when placing and
planning new facilities? These are all very important issues which are not
being researched.
_______________________________________________
H+T--Friends mailing list
H+T--Friends(a)ryoko.chrispy.net
http://ryoko.chrispy.net/mailman/listinfo/h+t--friends
5176
days inactive
5182
days old
12 comments
6 participants
participants (6)
-
 erik.weber@dot.gov
erik.weber@dot.gov -
 mbrenman001@comcast.net
mbrenman001@comcast.net -
 Phyllis Orrick
Phyllis Orrick -
 Ray, Renee
Ray, Renee -
 Reeves, Paula
Reeves, Paula -
 Sheryl Gross-Glaser
Sheryl Gross-Glaser